A Devastating Diagnosis with a Miraculous Recovery
The following events occurred between March 2017 and June 2018. Growing up, Kathy Karam, of Ocala, never intended to become a nurse. But when her husband,…

Update your location to show providers, locations, and services closest to you.
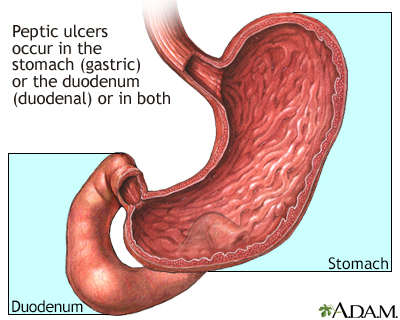
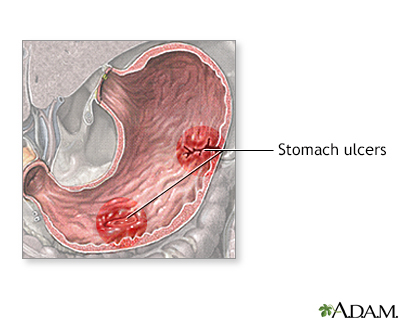
A peptic ulcer is an open sore or raw area in the lining of the stomach or intestine.
There are two types of peptic ulcers:
Ulcer - peptic; Ulcer - duodenal; Ulcer - gastric; Duodenal ulcer; Gastric ulcer; Dyspepsia - ulcers; Bleeding ulcer; Gastrointestinal bleeding - peptic ulcer; Gastrointestinal hemorrhage - peptic ulcer; G.I. bleed - peptic ulcer; H. pylori - peptic ulcer; Helicobacter pylori - peptic ulcer
Normally, the lining of the stomach and small intestines can protect itself against strong stomach acids. But if the lining breaks down, the result may be:
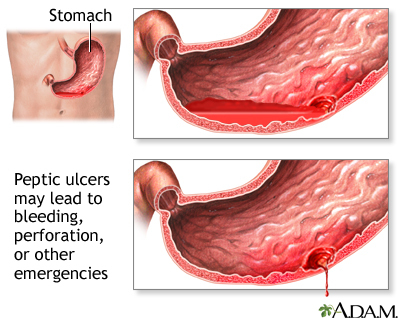
Most ulcers occur in the first layer of the inner lining. A hole in the stomach or duodenum is called a perforation. This is a medical emergency.
The most common cause of ulcers is infection of the stomach by bacteria called Helicobacter pylori (H pylori). Most people with peptic ulcers have these bacteria living in their digestive tract. Yet, many people who have these bacteria in their stomach do not develop an ulcer.
The following factors raise your risk for peptic ulcers:
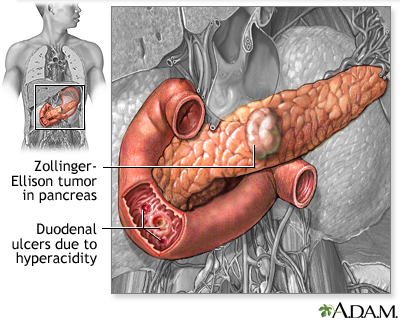
A rare condition, called Zollinger-Ellison syndrome, causes stomach and duodenal ulcers.
Small ulcers may not cause any symptoms. Some ulcers can cause serious bleeding.
Abdominal pain (often in the upper mid-abdomen) is a common symptom. The pain can differ from person to person. Some people have no pain.
Pain occurs:
Other symptoms include:
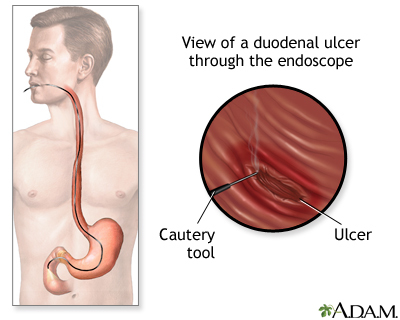
To detect an ulcer, you may need a test called an upper endoscopy (EGD).
EGD is done on most people when peptic ulcers are suspected or when you have:
Testing for H pylori is also needed. This may be done by biopsy of the stomach during endoscopy, with a stool test, or by a urea breath test.
Other tests you may have include:
Sometimes, you may need a test called an upper GI series. A series of x-rays are taken after you drink a thick substance called barium. This does not require sedation.
Your health care provider will recommend medicines to heal your ulcer and prevent a relapse. The medicines will:
Take all of your medicines as you have been told. Other changes in your lifestyle can also help.
If you have a peptic ulcer with an H pylori infection, the standard treatment uses different combinations of the following medicines for 7 to 14 days:
You will likely need to take a PPI for 8 weeks if:
Your provider may also prescribe this type of medicine regularly if you continue taking aspirin or NSAIDs for other health conditions.
Other medicines used for ulcers are:
If a peptic ulcer bleeds a lot, an EGD may be needed to stop the bleeding. Methods used to stop the bleeding include:
Surgery may be needed if:
Peptic ulcers tend to come back if untreated. There is a good chance that the H pylori infection will be cured if you take your medicines and follow your provider's advice. You will be much less likely to get another ulcer.
Complications may include:
Get medical help right away if you:
Contact your provider if:
Avoid aspirin, ibuprofen, naproxen, and other NSAIDs. Try acetaminophen instead. If you must take such medicines, talk to your provider first. Your provider may:
The following lifestyle changes may help prevent peptic ulcers:
Chan FKL, Lau JYW. Peptic ulcer disease. In: Feldman M, Friedman LS, Brandt LJ, eds. Sleisenger and Fordtran's Gastrointestinal and Liver Disease. 11th ed. Philadelphia, PA: Elsevier; 2021:chap 53.
Cover TL, Blaser MJ. Helicobacter pylori and other gastric Helicobacter species. In: Bennett JE, Dolin R, Blaser MJ, eds. Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases. 9th ed. Philadelphia, PA: Elsevier; 2020:chap 217.
Lanas A, Chan FKL. Peptic ulcer disease. Lancet. 2017;390(10094):613-624. PMID: 28242110 pubmed.ncbi.nlm.nih.gov/28242110/.

The following events occurred between March 2017 and June 2018. Growing up, Kathy Karam, of Ocala, never intended to become a nurse. But when her husband,…