Pyloric stenosis in infants
Definition
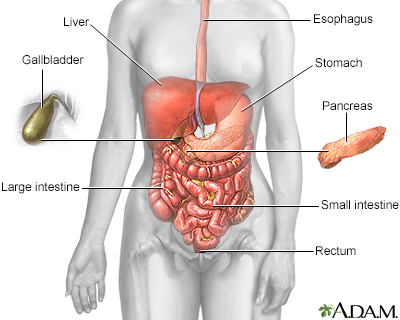
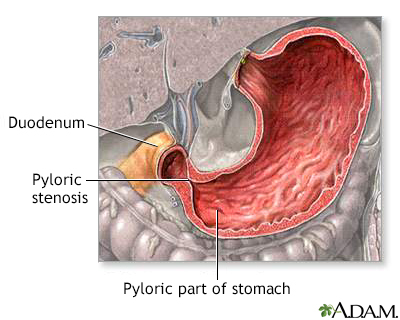
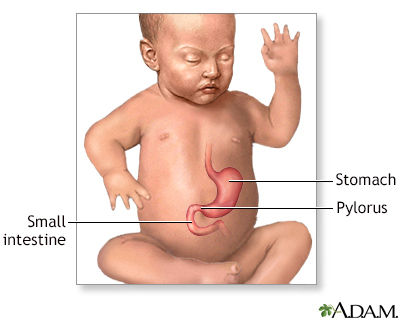
Pyloric stenosis is a narrowing of the opening from the stomach into the small intestine. This is called the pylorus. This article describes the condition in infants.
Alternative Names
Congenital hypertrophic pyloric stenosis; Infantile hypertrophic pyloric stenosis; Gastric outlet obstruction; Vomiting - pyloric stenosis
Causes
Normally, food passes easily from the stomach into the first part of the small intestine through a valve called the pylorus. With pyloric stenosis, the muscles of the pylorus are thickened. This prevents the stomach from emptying into the small intestine.
The exact cause of the thickening is unknown. Genes may play a role, since children of parents who had pyloric stenosis are more likely to have this condition. Other risk factors include:
- Certain antibiotics
- Too much acid in the first part of the small intestine (duodenum)
- Certain diseases a baby is born with, such as diabetes
Pyloric stenosis occurs most often in infants younger than 6 months. It is more common in boys than in girls.
Symptoms
Vomiting is the first symptom in most children:
- Vomiting may occur after every feeding or only after some feedings.
- Vomiting usually starts around 3 weeks of age, but may start any time between 1 week and 5 months of age.
- Vomiting is forceful (projectile vomiting).
- The infant is hungry after vomiting and wants to feed again.
Other symptoms appear several weeks after birth and may include:
- Abdominal pain
- Burping
- Constant hunger
- Dehydration (gets worse as vomiting gets worse)
- Failure to gain weight or weight loss
- Wave-like motion of the abdomen shortly after feeding and just before vomiting occurs
Exams and Tests
The condition is often diagnosed before the baby is 6 months old.
A physical exam may reveal:
- Signs of dehydration, such as dry skin and mouth, less tearing when crying, and dry diapers
- Swollen belly
- Olive-shaped mass when feeling the upper belly, which is the abnormal pylorus
Ultrasound of the abdomen may be the first imaging test. Other tests may include:
- Barium x-ray -- reveals a swollen stomach and narrowed pylorus
- Blood tests -- often reveal an electrolyte imbalance
Treatment
Treatment for pyloric stenosis involves surgery to widen the pylorus. The surgery is called pyloromyotomy.
If it is not safe to put the infant to sleep for surgery, an endoscope is used. This is a long, flexible tube with a camera and a tiny balloon at the end. The balloon is inflated to widen the pylorus.
In infants who cannot have surgery, tube feeding or medicine to relax the pylorus is tried.
Outlook (Prognosis)
Surgery usually relieves all symptoms. As soon as several hours after surgery, the infant can start small, frequent feedings.
Possible Complications
If pyloric stenosis isn't treated, a baby won't get enough nutrition and fluid. The child can become underweight and dehydrated.
When to Contact a Medical Professional
Contact your health care provider if your baby has symptoms of this condition.
Gallery
References
Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM. Pyloric stenosis and other congenital anomalies of the stomach. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. 21st ed. Philadelphia, PA: Elsevier; 2020:chap 355.
Seifarth FG, Soldes OS. Congenital anomalies and surgical disorders of the stomach. In: Wyllie R, Hyams JS, Kay M, eds. Pediatric Gastrointestinal and Liver Disease. 6th ed. Philadelphia, PA: Elsevier; 2021:chap 25.
