Uterine fibroids are one of the most common gynecologic diagnoses in women and the most common benign tumors of the uterus. The prevalence can be as high as 80% in African American women and up to 70% in white women (1). At UF Health Center of Excellence in Minimally Invasive Gynecology, we have a team of experts trained in the management of fibroids to provide you with world class care.
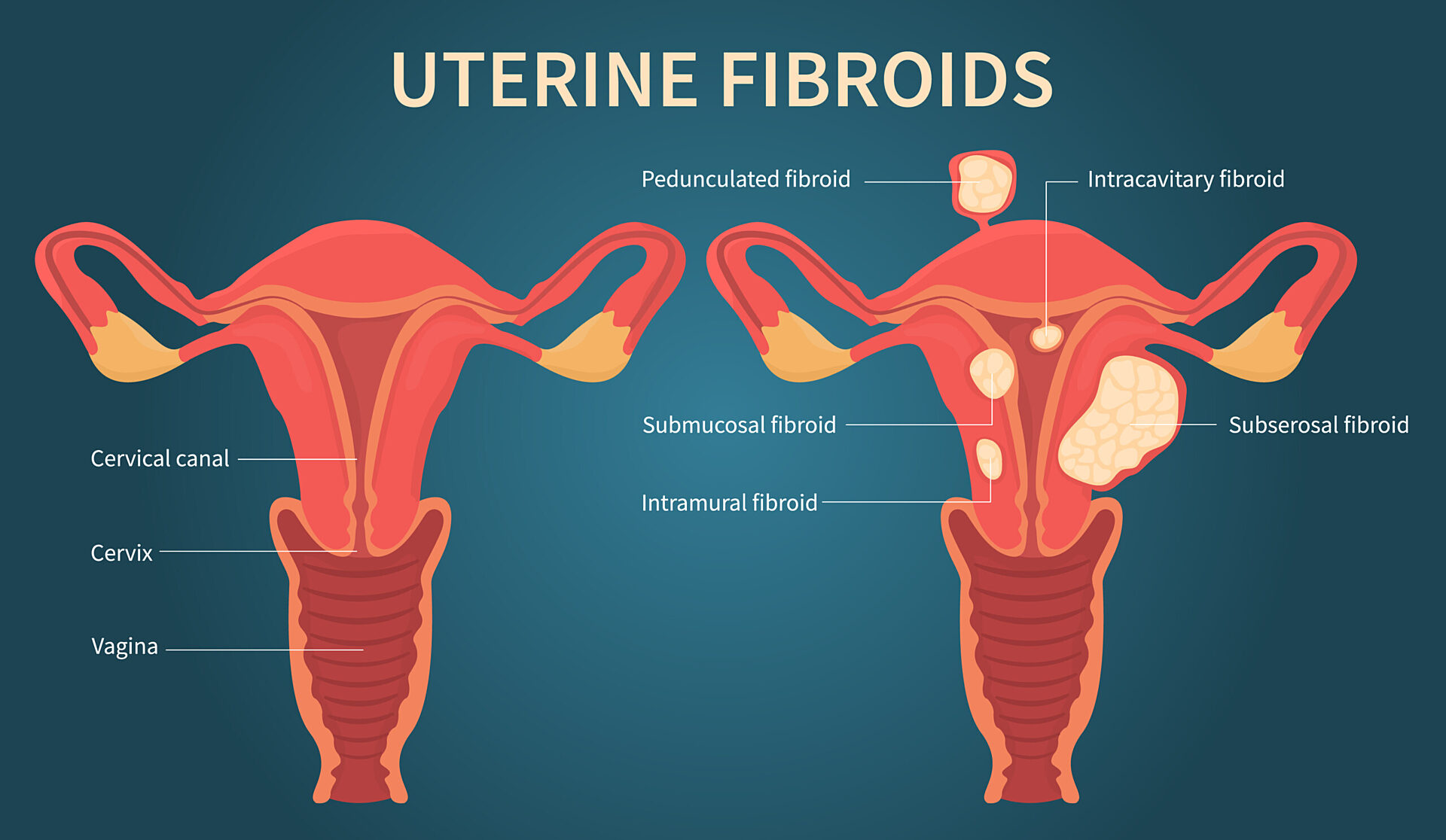
Uterine Fibroids Overview
As a result of their high prevalence, the impact of uterine fibroids is an important issue in women’s health. The financial burden of fibroids in the U.S. alone in 2012 was $34 billion (1).
The cost associated with uterine fibroids includes both direct medical expenses, such as surgeries, medications, medical visits, as well as indirect loss of income, including missed school and work days. Disparities exist in fibroid management, and African American women usually present a greater number and size of fibroids at a younger age. (1).
There is an inappropriate “normalization” of moderate to severe menstrual related symptoms that continues to be a problem in women’s care. Risk factors associated with fibroids are race, obesity, high blood pressure, early onset of periods, family history, older age and late menopause age. The cause of fibroids is largely unknown, with many theories involving hormones, epigenetic factors and stem cells, among other factors.
Around 30% of patients with fibroids may be symptomatic. Symptoms of fibroids can include a heavy period, anemia, pelvic pain and pelvic pressure, infertility, pregnancy complications, constipation and urinary frequency. Physical exams can diagnose moderate to large fibroids, but the first line diagnostic study is a pelvic ultrasound. Magnetic resonance imaging (MRI) can be useful especially for pre-surgical planning in women desiring to preserve their uterus.
Up to 70% of women have no symptoms and the fibroids are found incidentally. Asymptomatic patients don’t frequently require intervention. Surveillance can be done after a proper workup has been completed.
There are many available treatment options for fibroids. They can include observation, medical therapies, non-surgical interventions and surgery.
Our team of fellowship-trained minimally invasive gynecologic surgeons, Nash Moawad, MD, and Amira Quevedo, MD, have over 20 years of experience combined in fibroid care and are national and international speakers educating surgeons on ways to improve the quality of fibroid care for women worldwide. We treat most fibroid cases with a minimally invasive gynecologic surgery using no incision or small incisions, utilizing hysteroscopy, laparoscopy or robotic technology, allowing for less pain, less risk of adhesions, same day discharge and faster recovery.
Treatment may include watchful waiting in patients without symptoms, medications, radiologic interventional procedures and surgery. The surgical approach depends on the patient’s symptoms, the number, size and location of the fibroids and the patient’s desire for future fertility.
Medical therapies that can treat the fibroid symptoms of bleeding and pain include anti-inflammatories, tranexamic acid, levonorgestrel-intrauterine devices (IUDs) and oral contraceptives. Temporary volume reduction and symptom control can be achieved with medications called gonadotropin releasing hormone (GnRH) agonists and antagonists. GnRH analogs are not long-term options since they cause menopausal type symptoms and can lead to bone thinning over a long period of use. Because of this, we use GnRH in severe cases and special circumstances.
Interventional procedures such as uterine artery embolization (UAE) and magnetic resonance-guided focused radio frequency ablation (MRgFUS) are not recommended in women desiring future pregnancies because there is a risk of loss of ovarian and uterine function. These procedures are usually shorter, and recovery is usually faster than surgery. UAE and MRgFUS can be associated with post-embolization syndrome which leads to severe pain and fever requiring hospital admission. Furthermore, uterine artery embolization, may have a higher rate of complications including ischemic injuries and fibroid expulsion, therefore appropriate patient selection is the key to success. One in five women require further surgeries and recurrence of symptoms seems to be higher at 5 years.
Surgical options include myomectomy (removal of fibroids only) or hysterectomy (removal of the uterus and fibroids) depending on the woman’s personal desires and age. Ovaries are preserved in both approaches.
Myomectomy preserves the uterus for future childbearing. It has a high symptom improvement of 80%. Hysteroscopic removal of fibroids may be preferred in small fibroids that grow into the endometrial cavity of the uterus and does not require any incisions. We prefer the minimally invasive approaches including laparoscopic, robotic, and hysteroscopic techniques given faster recovery, shorter length of hospital stay, decreased pain, and decreased overall complications.
Depending on the number and location of the fibroids removed, it may be preferred to have a cesarean section prior to labor in future pregnancies. Recurrences of fibroids may be seen after myomectomy in 30% of women with a single fibroid or up to 50% of women with multiple fibroids over time. Typically, most of these surgeries are performed with same day discharge after surgery. Rarely, patients are admitted to the hospital for one to two days in complex cases. Complications of myomectomy are less than 5%, with recovery time usually 1-2 days after hysteroscopic surgery, up to two weeks after laparoscopic or robotic approach and up to six weeks if open surgery is required.
Hysterectomy is removal of the uterus and fibroids. It guarantees no future bleeding, periods and avoids the risk of recurrence of fibroids requiring further surgery. It does not change a woman’s hormones as the ovaries are typically spared. Hysterectomy is associated with significant improvement in the quality of life after surgery. Most women report improvement in intercourse with resolution in their bothersome period-related symptoms of bleeding, pain and pressure. We prefer again the minimally invasive approaches to hysterectomy including laparoscopic and robotic techniques with same day discharge, faster recovery, decreased pain, blood loss, improved patient satisfaction and decreased complications. A large fibroid uterus may carry a rare chance of cancer of less than 0.3%. We take every precaution and extract the fibroid uterus within a containment bag to prevent spread of potentially cancerous cells in these rare circumstances. Risk of major complications with hysterectomy in high volume centers like ours is less than 0.5%. Our surgeons take additional measures during surgery to decrease the risk of prolapse or descent of pelvic organs by supporting the vagina to strong ligaments in the pelvis at the time of the hysterectomy.
Laparoscopic radio frequency volumetric thermal ablation is a surgical laparoscopic technique under ultrasound guidance that ablates fibroids causing fibroid cellular death through small abdominal incisions. It has been associated with shrinkage of the fibroid volume of greater than 70% over six months. This is not recommended if you wish to get pregnant in the future because we don’t have enough studies yet regarding function of the uterus after this procedure.
Transcervical fibroid ablation is an outpatient procedure which ablates the uterine fibroids without requiring any incisions. It uses an ultrasound placed through the cervix into the uterus. Greater than 80% of symptom improvement was reported at 3 months with volume size reduction of 68% (2).
Endometrial ablation causes destruction of the endometrium or inside lining of the uterus. This is sometimes used in combination with hysteroscopic removal of the fibroid to achieve decrease in flow of heavy periods. Failure and re-operation can be seen in up to 40% of cases with fibroids. History of painful periods, larger fibroids, patients older than 45 years of age, and adenomyosis are risk factors for failure. One in four women will require further surgery after this procedure.
We believe in multidisciplinary, comprehensive, holistic approaches to care for our patients and their families who entrust us with their care. Our team is proactive in providing premier world class care with a tailored approach to suit each individual patient.
You can contact us for an individualized consultation or a second opinion if you have any of the following fibroid symptoms:
Anemia (low hemoglobin or blood counts) secondary to heavy periods
Pain during your period and during or after intercourse
Pelvic pressure symptoms on your bowel and bladder
Large fibroids and you have been told the only way is to do a large open procedure
Difficulty conceiving after 12 months of trying with your fibroids
Meet Our Team: Minimally Invasive Gynecologic Surgery
Obstetrician / Gynecologist (OBGYN), Women's Health Specialist
Languages: Spanish
Frequently Asked Questions About Uterine Fibroids
What are the main symptoms of uterine fibroids?
Uterine fibroid symptoms can include abnormal periods such as heavy or prolonged periods, painful periods, painful sex, pressure symptoms on your bladder such as urgency & frequent urination or on your rectum such as difficulty passing bowel movements.
Fibroids can increase the surface area of the endometrial cavity (the lining that sheds with your period every month) leading to heavier menstrual flow. Pain can be caused by inflammation associated with the rapid growth of fibroids, outpacing their blood supply.
How are uterine fibroids treated?
Asymptomatic fibroids can be observed and monitored with annual exams and ultrasounds. Abnormal uterine bleeding can be treated medically or surgically. Many hormonal options such as birth control pills, shots, vaginal rings, or hormonal intrauterine devices or implants can be used to control the bleeding. Other medications can prompt temporary menopause to control the bleeding and shrink the fibroids. Some medications work by improving the clotting mechanism to decrease the amount of bleeding with your periods.
If medical management is unsuccessful or contra-indicated, other options are available, such as uterine artery embolization (blocking the blood supply to the fibroids, performed by our Interventional Radiologists), or Radiofrequency ablation via hysteroscopy or laparoscopy. The fibroids can also be removed surgically, either with myomectomy or hysterectomy, depending on your symptoms, age, desire for future fertility and many other factors that are unique to you. Surgical removal of the fibroids can be performed via hysteroscopy (no incisions; if the fibroids are in the uterine cavity), or via small incisions in your abdomen, using laparoscopy or robot-assisted laparoscopy. Some fibroids require a larger incision. Even then, we try to use the smallest incision possible, such as Minilaparotomy in many cases. We offer you as many options as reasonable, and we tailor our approach to treatment options based on your unique situation and desires.
Do uterine fibroids cause infertility?
Uterine fibroids have been shown to negatively affect the implantation of pregnancies. Fibroids greater than 4-5 cm in the muscle of the uterine wall and any fibroids affecting the endometrial cavity (the implantation site of pregnancies) may be implicated in infertility and are frequently recommended for surgical removal to optimize the chances of successfully eliminating the fibroids. Removal of fibroids, also known as a myomectomy, is the preferred treatment modality in women wanting to conceive in the future or for those that have failed to get pregnant after 1 year of trying. Embolization or radio frequency ablation of fibroids is not recommended as the primary treatment for women wanting future pregnancies as they may impact fertility and future pregnancy outcomes.
How are uterine fibroids diagnosed?
You may be able to feel the fibroids in your abdomen if they are large. Fibroids may also be felt by your gynecologist during your exam. Your gynecologist will frequently order a pelvic ultrasound to confirm the findings and obtain further information. Often, an MRI is necessary if a myomectomy is considered, to gain further information regarding the location, number, and size of the fibroids. This is particularly useful to provide a roadmap of your fibroids and maximize the chance of removing as many of them as possible.
What are the risk factors for uterine fibroids?
Uterine fibroids are more common in women of African ancestry, in women with high blood pressure, obesity, early onset of periods, late age of menopause, older women, and women with a family history of fibroids. Older age greater than 40 years, family history, history of radiation therapy, and irregular features on ultrasound or MRI can raise the concern for malignancy in fibroids. We do not recommend myomectomy (removal of the fibroids with preservation of the uterus) in those cases. The risk of a cancer associated with a fibroid is overall low (less than 0.3%) and is highly dependent on the age of the patient. We are extremely diligent in carrying out the full workup before surgery to advise our patients to the best of our knowledge.
What does uterine fibroid pain feel like?
Uterine fibroid pain can vary from moderate to severe menstrual cramps to constant pressure symptoms in the lower abdomen, bladder, and rectal area. Most women will be able to ease fibroid-associated pain with over-the-counter medications such as anti-inflammatories. In some cases, women lose their quality of life or function with daily activities, and these are the patients that come to our practice seeking effective interventions.
What if I become pregnant and have fibroids?
If you have fibroids and become pregnant there is a good chance that you will have a healthy delivery without any complications.
Depending on the size and location of your fibroid(s) there is potentially an increased risk of preterm contractions, preterm delivery, increased bleeding during your delivery, breech presentation of the baby, or that you may require a cesarean section if you get pregnant with fibroids. Occasionally fibroids can grow significantly under the influence of pregnancy hormones, leading to increased pain and hospitalization.
References
Giuliani E, As-Sanie S, Marsh EE. Epidemiology and management of uterine fibroids. Int J Gynaecol Obstet. 2020 Apr;149(1):3-9. doi: 10.1002/ijgo.13102. Epub 2020 Feb 17. PMID: 31960950.
Shifrin G, Engelhardt M, Gee P, Pschadka G. Transcervical fibroid ablation with the Sonata™ system for treatment of submucous and large uterine fibroids. Int J Gynaecol Obstet. 2021 Oct;155(1):79-85. doi: 10.1002/ijgo.13638. Epub 2021 Mar 17. PMID: 33544889; PMCID: PMC8518813.
In February 2023, the UF Health Center of Excellence in Minimally Invasive Gynecologic Surgery program earned its Center of Excellence in Minimally Invasive…
Longtime faculty member and expert on women’s care selected as second Jacksonville faculty member to receive UF research award Andrew Kaunitz, M.D., is widely…