Thrombolytic therapy
Definition
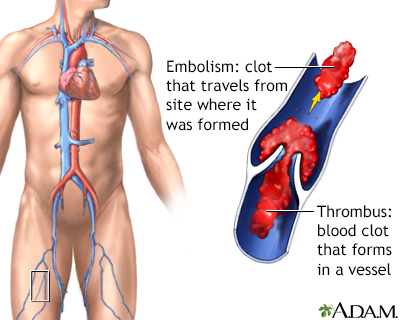
Thrombolytic therapy is the use of drugs to break up or dissolve blood clots, which are the main cause of both heart attacks and stroke.
Alternative Names
Tissue plasminogen activator; TPA; Alteplase; Reteplase; Tenecteplase; Activase thrombolytic agent; Clot-dissolving agents; Reperfusion therapy; Stroke - thrombolytic; Heart attack - thrombolytic; Acute embolism - thrombolytic; Thrombosis - thrombolytic; Lanoteplase; Staphylokinase; Streptokinase (SK); Urokinase; Stroke - thrombolytic therapy; Heart attack - thrombolytic therapy; Stroke - thrombolysis; Heart attack - thrombolysis; Myocardial infarction - thrombolysis
Information
Thrombolytic medicines are approved for the emergency treatment of stroke and heart attack. The most commonly used drug for thrombolytic therapy is tissue plasminogen activator (tPA), but other drugs can do the same thing.
Ideally, you should receive thrombolytic medicines within the first 30 minutes after arriving at the hospital for treatment.
Patient Education Video: Cardiac and vascular disorders: Blood clots
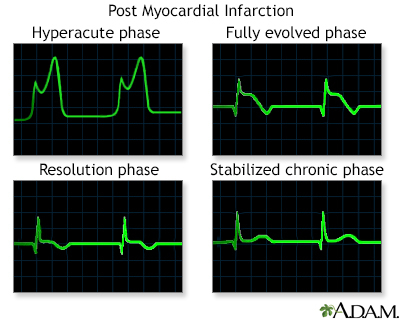
HEART ATTACKS
A blood clot can block the arteries to the heart. This can cause a heart attack, when part of the heart muscle dies due to a lack of oxygen being delivered by the blood.
Thrombolytics work by dissolving a major clot quickly. This helps restart blood flow to the heart and helps prevent damage to the heart muscle. Thrombolytics can stop a heart attack that would otherwise be larger or potentially deadly. Outcomes are better if you receive a thrombolytic drug within 12 hours after the heart attack starts. But the sooner treatment begins, the better the results.
The drug restores some blood flow to the heart in most people. However, the blood flow may not be completely normal and there may still be a small amount of muscle damaged. Further therapy, such as cardiac catheterization with angioplasty and stenting, may be needed.
Your health care provider will base the decisions about whether to give you a thrombolytic medicine for a heart attack on many factors. These factors include your history of chest pain and the results of an ECG test.
Other factors used to determine if you are a good candidate for thrombolytics include:
- Age (older people are at increased risk of complications)
- Sex
- Medical history (including your history of a previous heart attack, diabetes, low blood pressure, or increased heart rate)
Generally, thrombolytics may not be given if you have:
- A recent head injury
- Bleeding problems
- Bleeding ulcers
- Pregnancy
- Recent surgery
- Taken blood thinning medicines such as Coumadin
- Trauma
- Uncontrolled (severe) high blood pressure
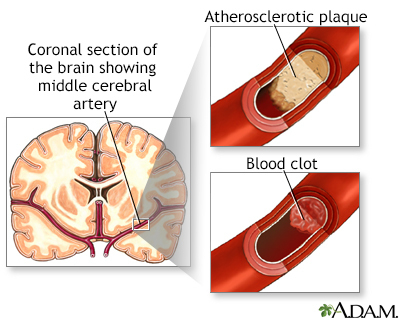
STROKES
Most strokes are caused when blood clots move to a blood vessel in the brain and block blood flow to that area. For such strokes (ischemic strokes), thrombolytics can be used to help dissolve the clot quickly. Giving thrombolytics within 3 hours of the first stroke symptoms can help limit stroke damage and disability.
The decision to give the drug is based upon:
- A brain CT scan to make sure there has not been any bleeding
- A physical exam that shows a significant stroke
- Your medical history
As in heart attacks, a clot-dissolving drug isn't usually given if you have one of the other medical problems listed above.
Thrombolytics are not given to someone who is having a stroke that involves bleeding in the brain. They could worsen the stroke by causing increased bleeding.
OTHER USES
Thrombolytic medications are sometimes used to treat other conditions including:
- Acute pulmonary embolism
- Clots in vascular catheters such as those used for dialysis
RISKS
Bleeding is the most common risk. It can be life threatening.
Minor bleeding from the gums or nose can occur in approximately 25% of people who receive the drug. Bleeding into the brain occurs approximately 1% of the time. This risk is the same for both stroke and heart attack patients.
If thrombolytics are felt to be too dangerous, other possible treatments for clots causing a stroke or heart attack include:
- Removal of the clot (thrombectomy)
- A procedure to open narrowed or blocked blood vessels that supply blood to the heart or the brain
CONTACT A HEALTH CARE PROVIDER OR CALL 911
Heart attacks and strokes are medical emergencies. The sooner treatment with thrombolytics begins, the better the chance for a good outcome.
Gallery
References
Bohula EA, Morrow DA. ST-elevation myocardial infarction: management. In: Libby P, Bonow RO, Mann DL, Tomaselli GF, Bhatt DL, Solomon SD, eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 12th ed. Philadelphia, PA: Elsevier; 2022:chap 38.
Jaffer IH, Weitz JI. Antithrombotic drugs. In: Hoffman R, Benz EJ, Silberstein LE, et al, eds. Hematology: Basic Principles and Practice. 7th ed. Philadelphia, PA: Elsevier; 2018:chap 149.
Kabrhel C. Pulmonary embolism and deep vein thrombosis. In: Walls RM, Hockberger RS, Gausche-Hill M, eds. Rosen's Emergency Medicine: Concepts and Clinical Practice. 10th ed. Philadelphia, PA: Elsevier; 2023:chap 74.
Kuo WT. Percutaneous interventions for acute pulmonary embolism. In: Mauro MA, Murphy KP, Thomson KR, Venbrux AC, Morgan RA, eds. Image-Guided Interventions. 3rd ed. Philadelphia, PA: Elsevier; 2021:chap 55.
O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127(4):529-555. PMID: 23247303 pubmed.ncbi.nlm.nih.gov/23247303/.
Papa L, Meurer WJ. Stroke. In: Walls RM, Hockberger RS, Gausche-Hill M, eds. Rosen's Emergency Medicine: Concepts and Clinical Practice. 10th ed. Philadelphia, PA: Elsevier; 2023:chap 87.