Egg donation
Egg donation offers many women with various infertility conditions a realistic chance of pregnancy.
Update your location to show providers, locations, and services closest to you.
Per American Society for Reproductive Medicine, infertility is a disease defined by failure to achieve successful pregnancy after 12 months or more of regular unprotected intercourse. Earlier evaluation and treatment may be justified based on medical history and physical findings and is warranted after 6 months for women over age 35 years.
In couples, about 50 percent of infertility problems are due to female factors; including ovulation dysfunctions, such as anovulation and other menstrual cycle abnormalities, as well as tubal, uterine and peritoneal factors, such as endometriosis. Male infertility accounts for about 30 percent of infertility in couples and the other 20 percent of couples may have a combination of both male and female gender-related factors. A specific reason cannot be identified using current technology for many patients with infertility problems. Fortunately, the majority of these couples with unexplained infertility will eventually have a successful pregnancy with a variety of treatment options.
Female age is a very important component of natural fertility. Apart from this, female infertility can be caused by ovulatory dysfunction (anovulation), tubal/uterine and peritoneal factors and some other unusual or unexplained factors.
Egg donation offers many women with various infertility conditions a realistic chance of pregnancy.
Most of the fertility promoting surgeries performed at UF Health use minimally invasive surgery techniques, allowing our patients to often go home on the same day.
Today young adult and pediatric survivors of cancer and other diseases are looking forward to a future of long-term survival due to improved treatments.
Endometriosis is a common disorder which is characterized by the presence of endometrial tissue implants that are outside the uterine lining.
Disorders of timely oocyte (egg) production are the most common causes of female infertility. These disorders range from anovulation, oligo-ovulation, to ovarian aging. Anovulation and oligo-ovulation are typically associated with cessation of regular menstrual cycles or longer time periods between menstrual cycles greater than 35 days. Many diseases are associated with anovulation and infertility.
Tubal factor can be acquired through pelvic inflammatory disease as a result of:
Some women may have a history of surgical sterilization procedure through bilateral tubal interruption. Through laparoscopy micro-surgical techniques can be applied to restore the issues with the fallopian tubes. If it cannot be treated surgically then In Vitro Fertilization will be the only option to conceive. Some women who underwent surgical sterilization may desire their tubes to be reconstructed. This procedure is called tubal reversal.
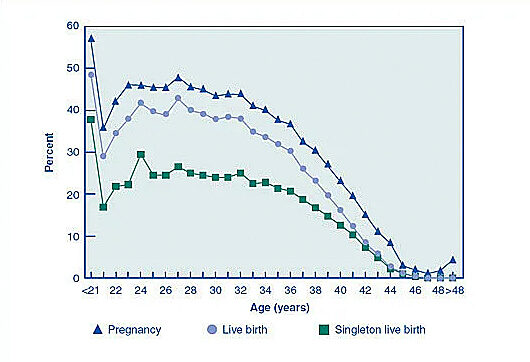
Female age is the most important parameter when it comes to natural fertility. We encourage couples to keep their “biological time clock” in mind, while planning to start a family.
Unexplained infertility is diagnosed when the couple has completed a through evaluation without finding a cause for infertility. Some unexplained infertility factors can be uncovered during an IVF cycle observing a low fertilization rate by conventional insemination. Many cases are probably related to multiple factors like somewhat advanced female age of above 35 or 37, semen analysis in low-normal range or advance male age of above 50 years. The treatment for these couples includes life style modifications, superovulation with or without intrauterine insemination and in vitro fertilization.