Definition
Ambiguous genitalia is a birth defect where the outer genitals do not have the typical appearance of either a boy or a girl.
Considerations
The genetic sex of a child is determined at conception. The mother's egg cell contains an X chromosome, while the father's sperm cell contains either an X or a Y chromosome. These X and Y chromosomes determine the child's genetic sex.
Normally, an infant inherits 1 pair of sex chromosomes, 1 X from the mother and 1 X or one Y from the father. The father "determines" the genetic sex of the child. A baby who inherits the X chromosome from the father is a genetic female and has 2 X chromosomes. A baby who inherits the Y chromosome from the father is a genetic male and has 1 X and 1 Y chromosome.
The male and female reproductive organs and genitals both come from the same tissue in the fetus. Ambiguous genitalia can develop if the process that causes this fetal tissue to become "male" or "female" is disrupted. This makes it hard to easily identify the infant as male or female. The extent of the ambiguity varies. Very rarely, the physical appearance may be fully developed as the opposite of the genetic sex. For example, a genetic male may have developed the appearance of a normal female.
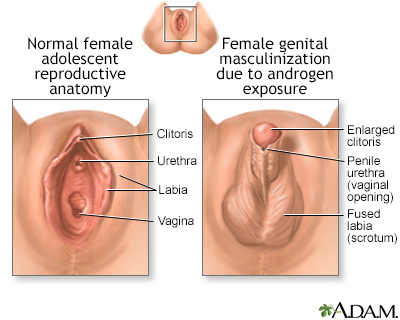
In most cases, ambiguous genitalia in genetic females (babies with 2 X chromosomes) has the following features:
- An enlarged clitoris that looks like a small penis.
- The urethral opening (where urine comes out) can be anywhere along, above, or below the surface of the clitoris.
- The labia may be fused and look like a scrotum.
- The infant may be thought to be a male with undescended testicles.
- Sometimes a lump of tissue is felt within the fused labia, further making it look like a scrotum with testicles.
In a genetic male (1 X and 1 Y chromosome), ambiguous genitalia most often include the following features:
- A small penis (less than 2 to 3 centimeters, or 3/4 to 1 1/4 inches) that looks like an enlarged clitoris (the clitoris of a newborn female is normally somewhat enlarged at birth).
- The urethral opening may be anywhere along, above, or below the penis. It can be located as low as the perineum, further making the infant appear to be female.
- There may be a small scrotum that is separated and looks like labia.
- Undescended testicles commonly occur with ambiguous genitalia.
With a few exceptions, ambiguous genitalia is most often not life-threatening. However, it can create social problems for the child and family. For this reason, a team of experienced specialists, including neonatologists, geneticists, endocrinologists, and psychiatrists or social workers will be involved in the child's care.
Causes
Causes for ambiguous genitalia includes:
- Pseudohermaphroditism. The genitalia are of one sex, but some physical characteristics of the other sex are present.
- True hermaphroditism. This is a very rare condition, in which tissue from both the ovaries and testicles is present. The child may have parts of both male and female genitals.
- Mixed gonadal dysgenesis (MGD). This is an intersex condition, in which there are some male structures (gonad, testis), as well as a uterus, vagina, and fallopian tubes.
- Congenital adrenal hyperplasia. This condition has several forms, but the most common form causes the genetic female to appear male. Many states test for this potentially life-threatening condition during newborn screening exams.
- Chromosomal abnormalities, including Klinefelter syndrome (XXY) and Turner syndrome (XO).
- If the mother takes certain medicines (such as androgenic steroids), a genetic female may look more male.
- Lack of production of certain hormones can cause the embryo to develop with a female body type, regardless of genetic sex.
- Lack of testosterone cellular receptors. Even if the body makes the hormones needed to develop into a physical male, the body cannot respond to those hormones. This produces a female body type, even if the genetic sex is male.
Home Care
Because of the potential social and psychological effects of this condition, parents should make a decision about whether to raise the child as a male or female early after diagnosis. It is best if this decision is made within the first few days of life. However, this is an important decision, so parents should not rush it.
When to Contact a Medical Professional
Contact your health care provider if you are concerned about the appearance of your child's external genitalia, or your baby:
- Takes more than 2 weeks to regain his or her birth weight
- Is vomiting
- Looks dehydrated (dry inside of mouth, no tears when crying, less than 4 wet diapers per 24 hours, eyes look sunken in)
- Has a decreased appetite
- Has blue spells (short periods when a reduced amount of blood flows into the lungs)
- Has trouble breathing
These can all be signs of congenital adrenal hyperplasia.
Ambiguous genitalia may be discovered during the first well-baby exam.
What to Expect at Your Office Visit
The provider will perform a physical exam which may reveal genitals that are not "typical male" or "typical female," but somewhere in between.
The provider will ask medical history questions to help identify any chromosomal disorders. Questions may include:
- Is there any family history of miscarriage?
- Is there any family history of stillbirth?
- Is there any family history of early death?
- Have any family members had infants who died in the first few weeks of life or who had ambiguous genitalia?
- Is there any family history of any of the disorders that cause ambiguous genitalia?
- What medicines did the mother take before or during pregnancy (especially steroids)?
- What other symptoms are present?
Genetic testing can determine if the child is a genetic male or female. Often a small sample of cells can be scraped from inside the child's cheeks for this testing. Examining these cells is often enough to determine the genetic sex of the infant. Chromosomal analysis is a more extensive test that may be needed in more questionable cases.
Endoscopy, abdominal x-ray, abdominal or pelvic ultrasound, and similar tests may be needed to determine the presence or absence of the internal genitals (such as undescended testes).
Laboratory tests may help determine how well the reproductive organs are functioning. This can include tests for adrenal and gonadal steroids.
In some cases, laparoscopy, exploratory laparotomy, or biopsy of the gonads may be needed to confirm disorders that can cause ambiguous genitalia.
Depending on the cause, surgery, hormone replacement, or other treatments are used to treat conditions that can cause ambiguous genitalia.
Sometimes, the parents must choose whether to raise the child as male or female (regardless of the child's chromosomes). This choice can have a big social and psychological impact on the child, so counseling is most often recommended.
Note: It is often technically easier to treat (and therefore raise) the child as female. This is because it is easier for a surgeon to make female genitalia than it is to make male genitalia. Therefore, sometimes this is recommended even if the child is genetically male. However, this is a difficult decision. You should discuss it with your family, your child's provider, the surgeon, your child's endocrinologist, and other health care team members.
References
Rey RA, Josso N. Diagnosis and treatment of disorders of sexual development. In: Jameson JL, De Groot LJ, de Kretser DM, et al, eds. Endocrinology: Adult and Pediatric. 7th ed. Philadelphia, PA: Elsevier Saunders; 2016:chap 119.
White PC. Congenital adrenal hyperplasia and related disorders. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. 21st ed. Philadelphia, PA: Elsevier; 2020:chap 594.
White PC. Sexual development and identity. In: Goldman L, Schafer AI, eds. Goldman-Cecil Medicine. 26th ed. Philadelphia, PA: Elsevier; 2020:chap 220.
Yu RN, Diamond DA. Disorders of sexual development: etiology, evaluation, and medical management. In: Partin AW, Dmochowski RR, Kavoussi LR, Peters CA, eds. Campbell-Walsh-Wein Urology. 12th ed. Philadelphia, PA: Elsevier; 2021:chap 48.