What pregnant women should know about Group B strep
Pregnant women undergo a variety of tests while they’re expecting. Although it’s not the most discussed test (that award would go to the glucose screening and…

Update your location to show providers, locations, and services closest to you.
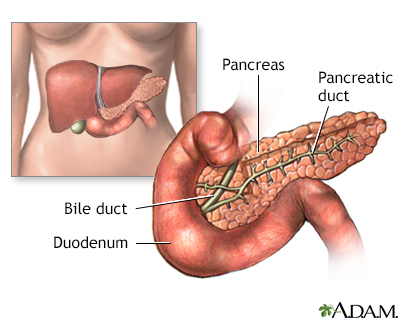
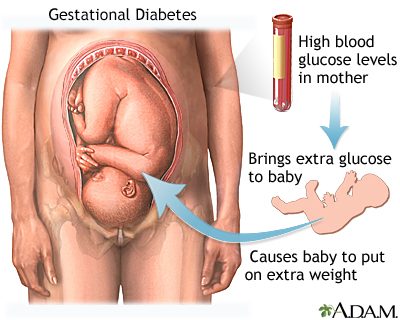
Gestational diabetes is high blood sugar (glucose) that starts or is first diagnosed during pregnancy.
Glucose intolerance during pregnancy
Pregnancy hormones can inhibit insulin from doing its job. When this happens, glucose level may increase in a pregnant woman's blood.
You are at greater risk for gestational diabetes if you:
Most of the time, there are no symptoms. The diagnosis is made during a routine prenatal screening.
Mild symptoms, such as increased thirst or shakiness, may be present. These symptoms are usually not dangerous to the pregnant woman.
Other symptoms may include:
Gestational diabetes most often starts halfway through the pregnancy. All pregnant women should receive an oral glucose tolerance test (glucose challenge test) between the 24th and 28th week of pregnancy to look for the condition. Women who have risk factors for gestational diabetes may have this test earlier in the pregnancy.
Once you are diagnosed with gestational diabetes, you can see how well you are doing by testing your glucose level at home. The most common way involves pricking your finger and putting a drop of your blood on a machine that will give you a glucose reading.
The goals of treatment are to keep blood sugar (glucose) level within normal limits during the pregnancy, and to make sure that the growing baby is healthy.
WATCHING YOUR BABY
Your health care provider should closely check both you and your baby throughout the pregnancy. Fetal monitoring will check the size and health of the fetus.
A nonstress test is a very simple, painless test for you and your baby.
If you take medicine to control diabetes, you may need to be monitored more often toward the end of your pregnancy.
DIET AND EXERCISE
In many cases, eating healthy foods, staying active, and managing your weight are all that are needed to treat gestational diabetes.
The best way to improve your diet is by eating a variety of healthy foods. You should learn how to read food labels and check them when making food decisions. Talk to your provider if you are a vegetarian or on another special diet.
In general, when you have gestational diabetes, your diet should:
Talk with your provider about the physical activities that are right for you. Low-impact exercises, such as swimming, brisk walking, or using an elliptical machine are safe ways to control your blood sugar and weight.
If managing your diet and exercising don't control your blood sugar, you may be prescribed diabetes medicine or insulin therapy.
There are many risks of having diabetes in pregnancy when blood sugar is not well controlled. With good control, most pregnancies have good outcomes.
Pregnant women with gestational diabetes tend to have larger babies at birth. This can increase the chance of problems at the time of delivery, including:
Your baby is more likely to have periods of low blood sugar (hypoglycemia) during the first few days of life, and may need to be monitored in a neonatal intensive care unit (NICU) for a few days.
Mothers with gestational diabetes have an increased risk for high blood pressure during pregnancy and increased risk for preterm delivery. Mothers with seriously uncontrolled blood sugar have a higher risk for stillbirth.
After delivery:
Contact your provider if you are pregnant and you have symptoms of diabetes.
Early prenatal care and having regular checkups helps improve your health and the health of your baby. Getting prenatal screening at 24 to 28 weeks of pregnancy will help detect gestational diabetes early.
If you are overweight, getting your weight within the normal body mass index (BMI) range will decrease your risk for gestational diabetes.
American Diabetes Association Professional Practice Committee; American Diabetes Association Professional Practice Committee; Draznin B, Aroda VR, Bakris G, et al. Management of diabetes in pregnancy: standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S232-S243. PMID: 34964864. pubmed.ncbi.nlm.nih.gov/34964864/.
Landon MB, Catalano PM, Gabbe SG. Diabetes mellitus complicating pregnancy. In: Landon MB, Galan HL, Jauniaux ERM, et al, eds. Gabbe's Obstetrics: Normal and Problem Pregnancies. 8th ed. Philadelphia, PA: Elsevier; 2021:chap 45.
Metzger BE. Diabetes mellitus and pregnancy. In: Jameson JL, De Groot LJ, de Kretser DM, et al, eds. Endocrinology: Adult and Pediatric. 7th ed. Philadelphia, PA: Elsevier Saunders; 2016:chap 45.
US Preventive Services Task Force, Davidson KW, Barry MJ, et al. Screening for gestational diabetes: US Preventive Services Task Force Recommendation Statement. JAMA. 2021;326(6):531-538. PMID: 34374716. pubmed.ncbi.nlm.nih.gov/34374716/.

Pregnant women undergo a variety of tests while they’re expecting. Although it’s not the most discussed test (that award would go to the glucose screening and…
October 14, 2014
Last week, we announced the creation of the UF Diabetes Institute. Given the many fundamental contributions of our faculty to this field over the years, the UF…
College of Dentistry, College of Medicine, College of Nursing, +3 more
For the millions of women in America who develop gestational diabetes during pregnancy, roughly 10% of all expectant moms, the health risks are real — both for them and their babies. Typically,...
Oh, the scourge of gestational diabetes. Doesn’t pregnancy inflict enough hardships on a woman’s body, with its aches, swelling, nausea, cravings, heartburn and sleepless nights? Must it also alter...
Baked, mashed or fried — any way you have them, potatoes are pure comfort food and a cause for cravings in some pregnant women. But women who are pregnant or looking to have a baby may want to keep...
