Otitis media with effusion
Definition
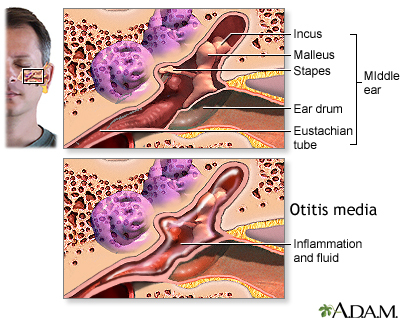
Otitis media with effusion (OME) is thick or sticky fluid behind the eardrum in the middle ear. It occurs without an ear infection.
Alternative Names
OME; Secretory otitis media; Serous otitis media; Silent otitis media; Silent ear infection; Glue ear
Causes
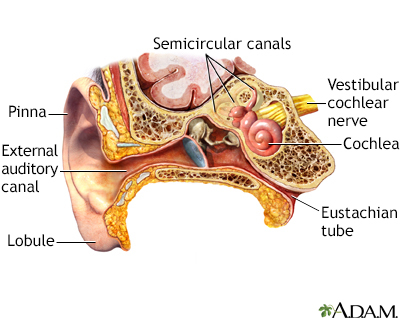
The Eustachian tube connects the inside of the ear to the back of the throat. This tube helps drain fluid to prevent it from building up in the ear. The fluid drains from the tube and is swallowed.
OME and ear infections are connected in two ways:
- After most ear infections have been treated, fluid (an effusion) remains in the middle ear for a few days or weeks.
- When the Eustachian tube is partially blocked, fluid builds up in the middle ear. Bacteria inside the ear become trapped and begin to grow. This may lead to an ear infection.
The following can cause swelling of the Eustachian tube lining that leads to increased fluid in the middle ear:
- Allergies
- Irritants (particularly cigarette smoke)
- Respiratory infections
The following can cause the Eustachian tube to close or become blocked:
- Drinking while lying on your back
- Sudden increases in air pressure (such as descending in an airplane or on a mountain road)
Getting water in a baby's ears will not lead to a blocked Eustachian tube.
OME is most common in winter or early spring, but it can occur at any time of year. It can affect people of any age. It occurs most often in children under age 2, but is rare in newborns.
Younger children get OME more often than older children or adults for several reasons:
- The tube is shorter, more horizontal, and straighter, making it easier for bacteria to enter.
- The tube is floppier, with a tinier opening that's easy to block.
- Young children get more colds because it takes time for the immune system to be able to recognize and ward off cold viruses.
The fluid in OME is often thin and watery. In the past, it was thought that the fluid got thicker the longer it was present in the ear. ("Glue ear" is a common name given to OME with thick fluid.) However, fluid thickness is now thought to be related to the ear itself, rather than to how long the fluid is present.
Symptoms
Unlike children with an ear infection, children with OME do not act sick.
OME often does not have obvious symptoms.
Older children and adults often complain of muffled hearing or a sense of fullness in the ear. Younger children may turn up the television volume because of hearing loss.
Exams and Tests
The health care provider may find OME while checking your child's ears after an ear infection has been treated.
The provider will examine the eardrum and look for certain changes, such as:
- Air bubbles on the surface of the eardrum
- Dullness of the eardrum when a light is used
- Eardrum that does not seem to move when little puffs of air are blown at it
- Fluid behind the eardrum
A test called tympanometry is an accurate tool for diagnosing OME. The results of this test can help tell the amount and thickness of the fluid.
The fluid in the middle ear can be accurately detected with:
- Acoustic otoscope
- Reflectometer -- a portable device
An audiometer or other type of formal hearing test may be done. This can help the provider decide on treatment.
Treatment
Most providers will not treat OME at first, unless there are also signs of an infection. Instead, they will recheck the problem in 2 to 3 months.
You can make the following changes to help clear up the fluid behind the eardrum:
- Avoid cigarette smoke
- Encourage infants to breastfeed
- Treat allergies by staying away from triggers (such as dust). Adults and older children may be given allergy medicines.
Most often the fluid will clear on its own. Your provider may suggest watching the condition for a while to see if it is getting worse before recommending treatment.
If the fluid is still present after 6 weeks, the provider may recommend:
- Continuing to watch the problem
- A hearing test
- A single trial of antibiotics (if they were not given earlier)
If the fluid is still present at 8 to 12 weeks, antibiotics may be tried. These medicines are not always helpful.
At some point, the child's hearing should be tested.
If there is significant hearing loss (more than 20 decibels), antibiotics or ear tubes might be needed.
If the fluid is still present after 4 to 6 months, tubes are probably needed, even if there is no major hearing loss.
Sometimes the adenoids must be taken out for the Eustachian tube to work properly.
Outlook (Prognosis)
OME most often goes away on its own over a few weeks or months. Treatment may speed up this process. Glue ear may not clear up as quickly as OME with a thinner fluid.
OME is most often not life threatening. Most children do not have long-term damage to their hearing or speaking ability, even when the fluid remains for many months.
When to Contact a Medical Professional
Contact your provider if:
- You think you or your child might have OME. (You should continue to watch the condition until the fluid has disappeared.)
- New symptoms develop during or after treatment for this disorder.
Gallery
References
Kerschner JE, Preciado D. Otitis media. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. 21st ed. Philadelphia, PA: Elsevier; 2020:chap 658.
Pelton SI. Otitis externa, otitis media, and mastoiditis. In: Bennett JE, Dolin R, Blaser MJ, eds. Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases. 9th ed. Philadelphia, PA: Elsevier; 2020:chap 61.
Rosenfeld RM, Shin JJ, Schwartz SR, et al. Clinical practice guideline: Otitis media with effusion executive summary (update). Otolaryngol Head Neck Surg. 2016;154(2):201-214. PMID: 26833645 pubmed.ncbi.nlm.nih.gov/26833645/.
Schilder AGM, Rosenfeld RM, Venekamp RP. Acute otitis media and otitis media with effusion. In: Flint PW, Francis HW, Haughey BH, et al, eds. Cummings Otolaryngology: Head and Neck Surgery. 7th ed. Philadelphia, PA: Elsevier; 2021:chap 199.
