Small bowel resection
Definition
Small bowel resection is surgery to remove a part of your small bowel. It is done when part of your small bowel is blocked or diseased.
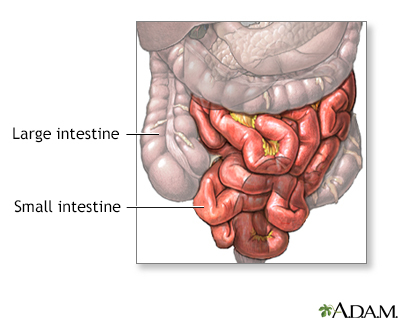
The small bowel is also called the small intestine. Most digestion (breaking down and absorbing nutrients) of the food you eat takes place in the small intestine.
Alternative Names
Small intestine surgery; Bowel resection - small intestine; Resection of part of the small intestine; Enterectomy
Description
You will receive general anesthesia at the time of your surgery. This will keep you asleep and pain-free.
The surgery can be performed laparoscopically or with open surgery.
If you have laparoscopic surgery:
- The surgeon makes 3 to 5 small cuts (incisions) in your lower belly. A medical device called a laparoscope is inserted through one of the cuts. The scope is a thin, lighted tube with a camera on the end. It lets the surgeon see inside your belly. Other medical instruments are inserted through the other cuts.
- A cut of about 2 to 3 inches (5 to 7.6 centimeters) may also be made if your surgeon needs to put their hand inside your belly to feel the intestine or remove the diseased segment.
- Your belly is filled with a harmless gas to expand it. This makes it easy for the surgeon to see and work.
- The diseased part of your small intestine is located and removed.
If you have open surgery:
- The surgeon makes a cut of 6 to 8 inches (15.2 to 20.3 centimeters) in your mid-belly.
- The diseased part of your small intestine is located and removed.
In both kinds of surgery, the next steps are:
- If there is enough healthy small intestine left, the ends are stitched or stapled together. This is called an anastomosis. Most patients have this done.
- If there is not enough healthy small intestine to reconnect, your surgeon makes an opening called a stoma through the skin of your belly. The small intestine is attached to the outer wall of your belly. Stool will go through the stoma into a drainage bag outside your body. This is called an ileostomy. The ileostomy may be either short-term or permanent.
Small bowel resection usually takes 1 to 4 hours.
Why the Procedure Is Performed
Small bowel resection is used to treat:
- A blockage in the intestine caused by scar tissue or congenital (from birth) deformities
- Bleeding, infection, or ulcers caused by inflammation of the small intestine from conditions such as Crohn disease
- Cancer
- Carcinoid tumor
- Injuries to the small intestine
- Meckel diverticulum (a pouch on the wall of the lower part of the intestine that is present at birth)
- Noncancerous (benign) tumors
- Precancerous polyps
Risks
Risks for anesthesia and surgery in general are:
- Reactions to medicines
- Breathing problems
- Blood clots, bleeding, infection
Risks for this surgery include:
- Bulging tissue through the incision, called an incisional hernia
- Damage to nearby organs in the body
- Diarrhea
- Problems with your ileostomy
- Scar tissue that forms in your belly and causes a blockage of your intestines
- Short bowel syndrome (when a large amount of the small intestine needs to be removed), which may lead to problems absorbing important nutrients and vitamins
- Chronic anemia
- The ends of your intestines that are sewn together come apart (anastomotic leak, which may be life threatening)
- Wound breaking open
- Wound infection
Before the Procedure
Tell your surgeon or nurse what medicines you are taking, even drugs, supplements, or herbs you bought without a prescription.
Talk with your surgeon or nurse about how surgery will affect:
- Intimacy and sexuality
- Pregnancy
- Sports
- Work
During the 2 weeks before your surgery:
- You may be asked to stop taking blood thinner drugs. These include aspirin, ibuprofen (Advil, Motrin), naproxen (Aleve, Naprosyn), and others.
- Ask the surgeon which drugs you should still take on the day of your surgery.
- If you smoke, try to stop. Smoking increases the risk for problems such as slow healing. Ask your doctor or nurse for help quitting.
- Tell your surgeon right away if you have a cold, flu, fever, herpes breakout, or other illness before your surgery.
- You may be asked to go through a bowel preparation to clean your intestines of all stool. This may involve staying on a liquid diet for a few days and using laxatives.
The day before surgery:
- You may be asked to drink only clear liquids such as broth, clear juice, and water.
- Follow instructions about when to stop eating and drinking.
On the day of surgery:
- Take the drugs your surgeon told you to take with a small sip of water.
- Arrive at the hospital on time.
After the Procedure
You will be in the hospital for 3 to 7 days. You may have to stay longer if your surgery was an emergency operation.
You also may need to stay longer if a large amount of your small intestine was removed or you develop problems.
By the second or third day, you will most likely be able to drink clear liquids. Thicker fluids and then soft foods will be added as your bowel begins to work again.
If a large amount of your small intestine was removed, you may need to receive liquid nutrition through a vein (IV) for a period of time. A special IV will be placed in your neck or upper chest area to deliver nutrition.
After you go home, follow instructions on how to take care of yourself as you heal.
Outlook (Prognosis)
Most people who have a small bowel resection recover fully. Even with an ileostomy, most people are able to do the activities they were doing before their surgery. This includes most sports, travel, gardening, hiking, and other outdoor activities, and most types of work.
If a large part of your small intestine was removed, you may have problems with loose stools and getting enough nutrients from the food you eat.
If you have a long-term (chronic) condition, such as cancer, Crohn disease or ulcerative colitis, you may need ongoing medical treatment.
Gallery
References
Albers BJ, Lamon DJ. Small bowel repair/resection. In: Baggish MS, Karram MM, eds. Atlas of Pelvic Anatomy and Gynecologic Surgery. 5th ed. Philadelphia, PA: Elsevier; 2021:chap 92.
Elmously A, Yeo HL. Management of small bowel obstruction. In: Cameron AM, Cameron JL, eds. Current Surgical Therapy. 13th ed. Philadelphia, PA: Elsevier; 2020:123-129.
Padilla PL, Khoo KH, Ho T, Cole EL, Sirvent RZ, Phillips LG. Small intestine. In: Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery. 21st ed. Philadelphia, PA: Elsevier; 2022:chap 69.
Related specialties
Aftercare and more
- Bathroom safety for adults
- Bland diet
- Crohn disease - discharge
- Ileostomy - caring for your stoma
- Ileostomy - changing your pouch
- Ileostomy - discharge
- Ileostomy - what to ask your doctor
- Ileostomy and your child
- Ileostomy and your diet
- Low-fiber diet
- Preventing falls
- Small bowel resection - discharge
- Surgical wound care - open
- Types of ileostomy
- Ulcerative colitis - discharge
- When you have nausea and vomiting
