
Successful spine surgery has patient living pain free
Sharon Meeks has spent her life taking care of her family. She and her husband were married for 55 years. They raised three children and worked hard on their…

Update your location to show providers, locations, and services closest to you.
Neurosurgeons at the University of Florida treat patients with spinal deformities like scoliosis and kyphosis.

We are proud to care for patients at UF Health Shands Hospital, ranked as one of the nation's top hospitals for neurology and neurosurgery by U.S. News & World Report..
Infantile Scoliosis occurs in children less than 3 years of age and is most commonly associated with other serious congenital or neurodegenerative disorders like cerebral palsy, tethered spinal cord, and myelomeningoceles, among others. Surgery is sometimes necessary, but often non-operative techniques are used to allow for spinal growth prior to a spinal fusion procedure.Scoliosis is an abnormal curvature of the spine that can occur in any age group. Scoliosis is a coronal plane (i.e. side to side) deformity occurring in children, adolescents, and adults. Symptoms vary with age of onset and severity of the curvature; cosmetic problems including sitting imbalance, breathing difficulty or delayed development is common findings in infants and young children. A rib hump, pelvic or shoulder height imbalance tend to common in the adolescent group. Intractable back pain, sciatica, leg weakness or numbness and gait difficulty are common reasons for surgical correction in adults.

Kyphosis is seen when a person's spinal balance has moved too far forward to allow the spine to effectively carry the body weight without progressive deformity, pain or neurologic loss of function. Patients typically walk in a forward flexed posture being unable to stand up straight. This condition can also occur along with scoliosis causing Kyphoscoliosis.
Treatment recommendations are made based on a combination of the severity of the curvature of the spine, the impact on the patient's ability to function on a day-to-day basis, their age and other medical conditions. In very selected cases in younger, cosmetic appearance is a reason for surgery. In general the treatment should match the magnitude and risks of the symptoms.
Bracing: In more mild forms of spinal deformities, bracing may be an option for younger patients where the spine may be .encouraged. to grow straighter. Adults may get some relief of pain with a brace, but it will not correct the deformity. Bracing may cause some problems like skin irritation or muscle disuse.
Physical Therapy: A mainstay of treatment is the flexibility and core strengthening of the spine, which can be enhanced by Physiotherapy (PT). There are many acceptable forms of PT, but they all share an active component where the patient exercises and strengthens the spinal musculature, improves range of motion and balance. It should be an active process, not simply limited to passive modalities like heat, ice or massage.
Pain Management Injections: T he injection of cortisone and similar medications with can offer temporary of focal relief of pain from mild nerve compression or joint arthritis. The injections are frequently repeated in groups of three and can only be given safely once or twice per year because of the side effects of the medications.
Surgical Correction: Prior to considering surgery, the typical patient should have tried and failed to manage their symptoms with non-operative treatments. Surgery should be considered in patients whose pain in medically refractory, or have neurologic symptoms including weakness, numbness or bowel or bladder dysfunction. Progressive worsening of the curvature is a common reason for surgery, and is the reason that patients are followed with yearly x-rays. Severe curves are felt to be unstable and tend to worsen despite all efforts at non-operative treatment; like a tree falling over, beyond a certain point it cannot be stopped without intervention.

Preoperative X-ray of a young patient with previous lumbar fusion surgery resulting in a Flat Back Syndrome; unable to walk upright or stand; with disabling pain

Preoperative X-ray of an elderly patient with progressive scoliosis since childhood. The severity of the curvature had progressed and become painful.
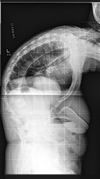
Preoperative X-ray of a patient with Ankylosing Spondylitis who was unable to stand up and could not look above the ground level.

The same patient as above, 2 years postop with improved balance and normal ability to stand upright, back to work full time.

Postoperative X-rays of the same patient showing correction of the curvature.

Postoperative X-ray of the same patient, now looking straight ahead.
Posterior fusion with spinal instrumentation is the most common procedure for the correction of scoliosis. Metal rods are anchored to the vertebra with screws and hooks (Titanium or Steel) in order to straighten and hold the spine in place. If there is a severe deformity, a cut is made in the bone, an Osteotomy, in order to realign the spine into a more normal orientation.
Anterior spinal fusions are also done for the correction of scoliosis. These are usually the more severe cases and are most commonly performed along with a posterior operation.
Sharon Meeks has spent her life taking care of her family. She and her husband were married for 55 years. They raised three children and worked hard on their…