Patient education
A traumatic injury of the spinal cord can lead to spinal cord injury (SCI), which can be characterized by a bruise or a tear of the spinal cord. Depending where the injury is and how severe it is, partial or complete loss of feeling and control in just the arms (paraplegia) or both the arms and legs (tetraplegia) may be present.
An estimated 12,000 SCIs occur annually as a consequence of auto accidents, acts of violence, falls, and sports injuries. Most spinal cord injuries occur in young people between the ages of 16-30, with the vast majority of those being males. The paralysis that follows an SCI is usually sudden. There may also be breathing, blood pressure problems, or problems controlling the bladder and bowel. Initial treatment may include surgery to maintain spine stability, breathing devices or specialized programs and equipment to prevent injury to the skin while in bed. Many SCI patients experience difficulty controlling urinating or bowel movements.
At UF, the Physiatry team will collect information about how the injury occurred, which may help to determine injury severity and if there are other associated injuries. At the Inpatient Rehabilitation Hospital, the Attending Physician will first perform a thorough examination including checking strength, reflexes, and sensation. The initial examinations may help to predict long term recovery from SCI. Precautions may be taken to prevent movement of the spine during the evaluation. The clinical care team will use Imaging of the spine and blood tests to assess if bleeding, infection or chemical abnormalities are present. If a brain injury also occurred, tests of thinking and other additional tests may take place.
Rehabilitation
The primary goals of rehabilitation are to inform the patients and families with education about SCI, improve function and prepare the patient for return to the community. Safety precautions will be taught to prevention of further injury or complications. Patient and families will receive education and training on performing bowel and bladder programs. Physical therapy and occupational therapy work with strengthening, stretch and mobility and helping the patient learn techniques for self-care. Assistive devices, ramps, and other changes in the environment may also be helpful. Medications may be used to address disorders that may be associated with SCI such as spasticity, depression and pain. Recovery depends on how severe the injury is, but most improvement is seen in the first 6 months after the injury. After the initial rehabilitation process, our Physiatrists will work with patients for long-term care needs.
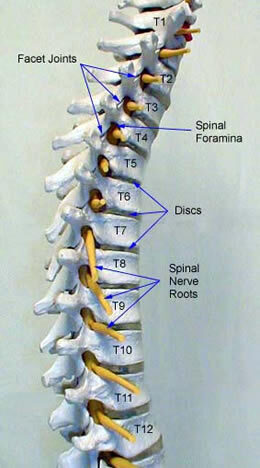

Spinal Anatomy
The spinal cord is a neural structure that extends from the base of the brain, down the middle of the back, to level of the waist. The spinal cord carries nerve fibers from the brain to nerve cells at each level of the cord. The fibers from these segmental nerve cells leave the cord through the spinal nerves. These spinal nerves exit at each vertebral level and communicate with specific areas of the body. There are both motor and sensory portions of the spinal nerves.
Rings of bone called vertebrae surround the spinal cord. The stacked vertebrae create the spinal column, which provide the support for the body. There are seven cervical vertebrae. The cervical bones are designed to allow flexion, extension, and rotation of the head. In the chest region, the thoracic spine attaches to the ribs. There are twelve vertebrae in the thoracic region. There are five vertebrae in the lumbar spine. The lowest lumbar vertebra articulates with the sacrum. The sacrum attaches to the pelvis.
Types of Spinal Cord Injury
SCI is the result of damage to the spinal cord from severing, stretch, or compression.
SCI can be divided into two types:
- complete and
- incomplete.
A complete injury means that there is no function below the level of the injury, i.e. no sensation and no voluntary movement. An incomplete injury means that there is some function below the primary level of the injury. A person with an incomplete injury may be able to move one limb or may be able to feel parts of the body that cannot be moved. The type of SCI is important in prognosis and return of function. Complete injuries tend to have little recovery, while incomplete injuries usually have some degree of improvement.
Causes and risk factors
Traumatic spinal cord injuries are caused by a sudden and severe hit to the spine. An overwhelming number of cases in which people suffer spinal cord trauma are tied to motor vehicle accidents and slips or falls. Other causes are violent acts, sports-related injuries and medical procedures, among others.
Among children, there are other well-documented causes such as birth injuries, trampoline accidents and diving accidents.
Most spinal cord injuries happen as a result of these types of traumatic events, as opposed to non-traumatic events that come about gradually from internal damage to the spinal cord region (infections, cancer/tumors, congenital medical issues, etc.).
Symptoms According to SCI Level
In general, the higher in the spinal column the spinal cord injury occurs, the more neurological dysfunction a person will experience.
Injuries between C-1 and C-4 are very critical because they impair the ability to breath. C-5 injuries result in good shoulder and biceps control, but no control at the wrist or hand and legs. C-6 injuries generally yield wrist control, but no hand or leg function. Individuals with C-7 and T-1 injuries can straighten their arms but still have dexterity problems with the hand and fingers. Injuries at the thoracic level and below result in paraplegia, with the hands not affected. High lumbar injuries affect the ability of the hip to flex and extend the legs, while lower lumbar injuries affect the mobility of the lower parts of the leg.
Often with SCI there is significant loss of bowel or bladder function. This can occur with injuries at any level. Sexual functioning is frequently affected by SCI. Other effects of SCI may include inability to regulate blood pressure effectively, reduced control of body temperature, inability to sweat below the level of injury, and chronic pain.
Diagnosis
The diagnosis of SCI is made by a detailed neurological examination. Plain radiographs and CT scans of the spine will show any significant fractures of the bones. MRI of the spine will show any injury to the actual spinal cord.
Treatment of Spinal Cord Injury
Because of the force that is required to fracture the spine, many spinal cord-injured patients suffer have significant associated injuries in the chest or abdomen. For isolated spinal cord injuries the mortality after one year is about 5-7%. If a patient survives the first 24 hours after spinal cord injury, the likelihood of survival for ten years is approximately 75-80%.
The immediate treatment of SCI is stabilization of the spine to prevent any further injury to the spinal cord. Within the first 24 hours, steroid drugs such as methylprednisolone are used to reduce swelling in the spinal cord. The benefit of steroids is limited and it has been shown to be useful only for a 24-hour period.
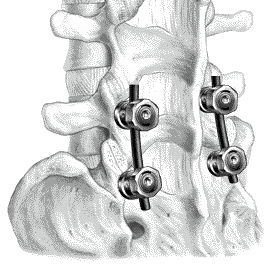
Surgery is indicated when there is significant instability of the spine or if there is compression of the spinal cord with an incomplete SCI. This may be a result of fractured bones or hematomas. Severe fractures may involve several columns of support in the spine, which will require surgical fixation to regain stability. Surgical fixation involves both instrumentation and fusion. Fusion is the joining of two vertebrae with bone graft (either from the patient or from cadaver) held together with metal hardware such as plates, rods, hooks, screws, and cages. The goal of the bone graft is to join the vertebrae above and below to form one solid piece of bone. It may take several months or longer to create a solid fusion. The instrumentation holds the bones together while the fusion is taking place.
Once stabilized, the goal of SCI treatment is rapid rehabilitation with the help of physical medicine specialists, physical therapists, occupational therapists, psychologists, and social workers. Patients must have a strong social support system to help them cope with their injury and relearn how to perform daily activities.